Reference: 二階老趙外科學
1. 腸造廔:最常見ileostomy,位於RLQ腹直肌較高處,外翻-->避免retraction
- 永久性: end
- 暫時性: loop or divided
2. 噤便肌肉:
- 尺骨直腸肌(骨骼肌):構成肛管直腸角度最重要的肌肉
- 內括約肌(85% resting pressure)
- 外括約肌深部 (骨骼肌)
3. 大腸生理
- 菌叢
- Bacteroides: 10^11 /ml
- E. coli: 10^9 /ml
- Layers: 上皮->lamina propria->黏膜肌層->submucosa->muscle layer->serosa
- 功能
- 吸收水分(10%):受aldosterone影養
- 留鈉排鉀,留氯排重碳酸
- 吸收短鏈脂肪酸
- 生理性息肉(=增生,占90%)
- 正常大腸上皮4~7七天換血
- 沒有惡性傾向,大多0.5cm以下,乙狀結腸/直腸最多
- 反應性息肉(=發炎)
- 好發:IBD
- 滯留性息肉(=錯構瘤、先天性)
- 好發:PJ症候群、幼年單發性息肉、幼年多發性息肉(25%癌變)
- 症狀:阻塞、出血
- 小兒下消化道出血最常見的原因
- 腫瘤(8%): 一般人發現息肉~癌變約52~62y/o
- tubular: 發生率最高,癌變5%
- tubulovillous
- villous: 發生率最少,癌變40%
- <1cm: 癌變1%
- >2cm: 癌變50%
- Familiar polyposis syndrome
- adenomatous: 癌變100%,related to ch.5(APC gene: tumor suppression),體顯性,發現~癌變約29~39 y/o
- polyposis coli
- Gardner's syndrome: related to 軟組織(fibroma)+骨頭(osteoma),periampullary cancer↑
- Turcot syndrome: related to CNS tumor
- harmatomatous
- PJ syndrome: GI癌變風險增加(2~13%)
- Diffuse juvenile polyposis: 癌變25%
- 息肉處理:endoscopic polypectomy(有stalk超過1.5cm)、可先注射N/S墊高病灶,拿下後看margin clear/no submucosa invasion/grade I~II(well to moderate differentiation)就不用切大腸,除非很多、很大或是villous type;大腸鏡complication: 穿孔(0.2%)、出血(1%)


- 家族遺傳性占15%,一等親罹癌則風險增3~9倍,偶發性85%
- normal-(APC,ch5)->dysplasia-(DNA hypomethylation)->early adenoma-(RAS,ch12,oncogene)->intermediate adenoma-(DCC,ch18,抑制基因)->late adenoma-(p53,ch17,抑制基因)->adenocarcinoma
- Initiation(1st): FAP(1%,癌化100%)
- Promotion: HNPCC(14%,癌化80%,較年輕約44y/o,right>left side,poor differentiated/signet ring type多,相同stage預後較佳,子宮內膜癌30~60%/乳癌↑/前列腺癌↑)

- Malignant change(last): 需biopsy confirmation
- CT/PET 看淋巴、肝臟轉移
- EUS看深度
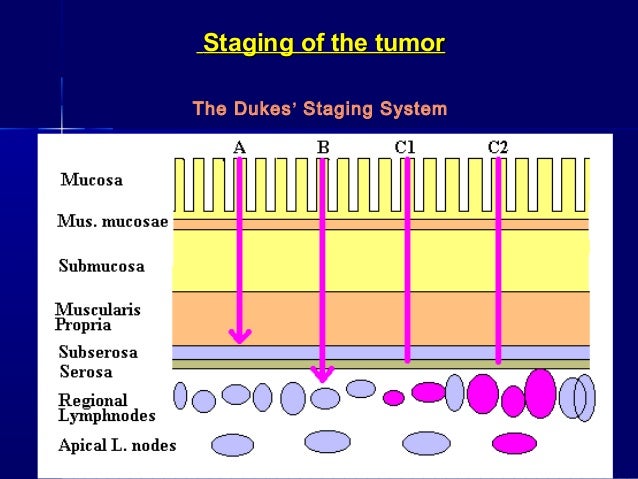
- TMN system
- stage I: T1~2N1M0= A+B1
- stage II: T3~4N0M0= B2+B3
- stage III: TanyN1~2M0= C1+C2+C3
- stage IV: M1= D
- 開刀
- safe margin: 2~5cm
- Pre-op: colon prepare; lavage before anastomosis or colostomy for 6~8wks(=Hartmann procedure) if emergent OP(left side)
- APR+ 永久性stomy
- LAR+ 保留直腸
- Adjuvant therapy
- chemo: oral 5-FU, levamisole(佐劑) or leukovorin
- radiation: only for rectal cancer


- UC 10~30%癌化
- bimodal distribution in age
- manifestation: bloody diarrhea
- evaluation of score: 體重是否下降、大便次數、心跳、血比容、發燒、ESR、albumin
- mild to moderate: ASA
- severe: total proctocolectomy+ ileal pouch anal anastomosis if intractable, toxic megacolon
- Crohn 7%狹窄處癌化
- 女>男,年輕人較多
- 可見cobblestone
- triad: abdominal pain, diarrhea, mild obstruction
- treatment: 5-ASA--> steroid--> azathioprine
- resection of complicated segment only: fistula/abscess(25%)> toxic megacolon(19%)> obstruction(12%)> perforation(<10%)
- Toxic megacolon
- T colon> 6cm + systemic toxic signs(+)
- Bowel rest, give antibiotics/steroid, avoid enema, then may arrange OP
- sigmoid(80%): elders with stool compaction
- cecum(15%): younger, cannot fix well
- 影像:inverted U shape+ bird peak colon gas on plain film
- 處理:排除peritoneal sign後,採取enema、肛管、endoscopic detorsion(成功率80%, 復發率40%)、elective operation(elective: 6~8wks後)包括right side hemicolectomy/cecopexy/ileocolostomy
7. Colon diverticulum
- at mesenteric side (反向: Meckel's, intestinal)
- pseudodiverticulum: lacking muscle layer
- diverticulosis: no infection, no inflammation, bleeding(+)
- 最常見成人大量LGI bleeding(24hr超過1500c.c.)的原因,其次是vascular ectasia、colon cancer
- 最常見兒童大量LGI bleeding的原因則是polyp
- 檢查出血位置:monitors, on NG, endoscope, Tc99m(0.1c.c./min), tagged RBC(0.5c.c./min), angiography(0.5~1.0c.c./min), operation
- diverticulitis: infection/inflammation(+),暫時不做endocscope
- uncomplicated: mild(pain)/severe(SIRS)
- 輕症發作兩次--> 開刀
- 重症發作一次--> 開刀
- 48hrs內未改善的腹痛-->考慮手術
- complicated: perforation/abscess(OP最常見的原因)/fistula(膀胱陰道)/obstruction
8. Radiotherapy induced proctitis
- 常見於cervical CA, prostate CA, bladder CA
- 劑量: 6000 cG
- 風險:老年、糖尿病
- 黏膜層(vomiting, diarrhea)-->血便(hematochesia)
9. 痔瘡
- 好發於3' 7' 11' 方位
- 以dentate line(pectinate line)分內外痔
- 內:vessel distention,出血+不痛
- 外:thrombosis,疼痛--> 48hrs內拿掉,或保守治療(軟便+高纖+溫水坐浴)
- 混合(最常見)
- 治療:
- 1~2度保守治療
- 2~3度結紮
- 3~4度hemorrhoidectomy(close有縫合, open不縫合, circumferential黏膜層+黏膜下層整圈=Whitehead's procedure)

- 術後注意事項
- 尿滯留(疼痛導致)
- 出血
10. Anal fissure
- dentate line以下
- 6' 占90%, 12' 占10%, lateral 要懷疑Crohn's disease
- 開刀時機:慢性肛裂(1個月),做單側lateral internal sphincterotomy(括約肌外側切開術)
- 風險因子: 女>男,老>少,做過子宮切除術、長期便秘
- types of prolapse
- 假的prolapse =mucosa only= 大規模內痔
- 真的prolapse= whole layer
- 評估:sphincter tone
- normal--> resection of prolapsed part
- bad-->
- proctopexy+/- sigmoid resection(anterior resection proctopexy)
- Ripstein procedure: transabdominal proctopexy + sling
- Delorme procedure(低風險): perineal approach, mucosa proctectomy
- Altemeier procedure: perineal approach, +resection
- Thiersch procedure
- 術後anal tone正常:60~70%
- 年輕男生多
- 薦骨尾骨下段3cm,與肛門直腸系統無關
- 容易藏汙納垢、感染發炎,需I&D,6~8wks後excision
13. Anal carcinoma
- 分類
- dentate line以下:SCC, BCC, melanoma
- dentate line以上:small cell carcinoma, SCC
- 治療:1st line- chemoradiation(5FU+ mitomycin C+3000rad)
14. Perianal abscess (gland感染)
- 容易有fistula
- 好發位置:intersphincter(60%), transphincter(35%), suprasphincter(4%), extrasphincter(1%)
- 處理:fistulotomy、seton drainage(2~3 months, 減少括約肌傷害)


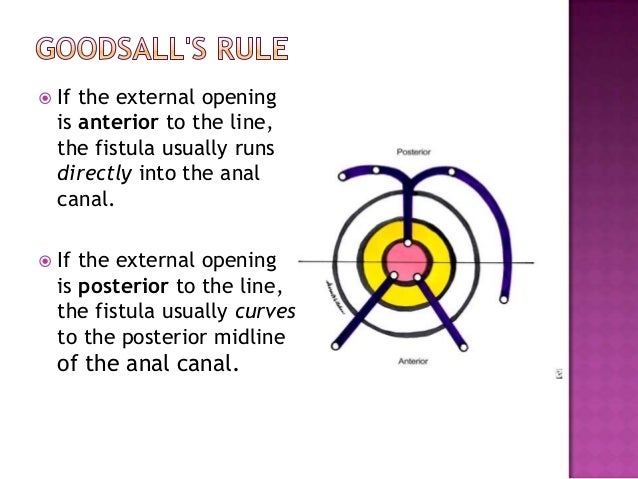
- Goodsall's rule 或施打methyl blue 找tract 路徑



沒有留言:
張貼留言