Stroke
1. Categories
- ischemic: 4/5
- atherosclerosis of large vessels, RFs: HTN, DM, hyperlipidemia
- lacunar stroke at small vessels(<1.5 cm on CT), RFs: HTN, DM
- cardiogenic embolism(multiple, unusual, distal sites, RFs: valvular diseases, MI, arrhythmia, rheumatic, op hx
- hemorrhagic: 1/5
2. Stenosis level
- severe stenosis: >70%
3. Stroke symptoms
- FAST: facial asymmetry, arm drop, slurred speech, time on onset
- motor: treat this part first!
- sensory
- consciousness, cognition etc.
* unspecific symmetric symptom: less likely due to stroke
4. NE:
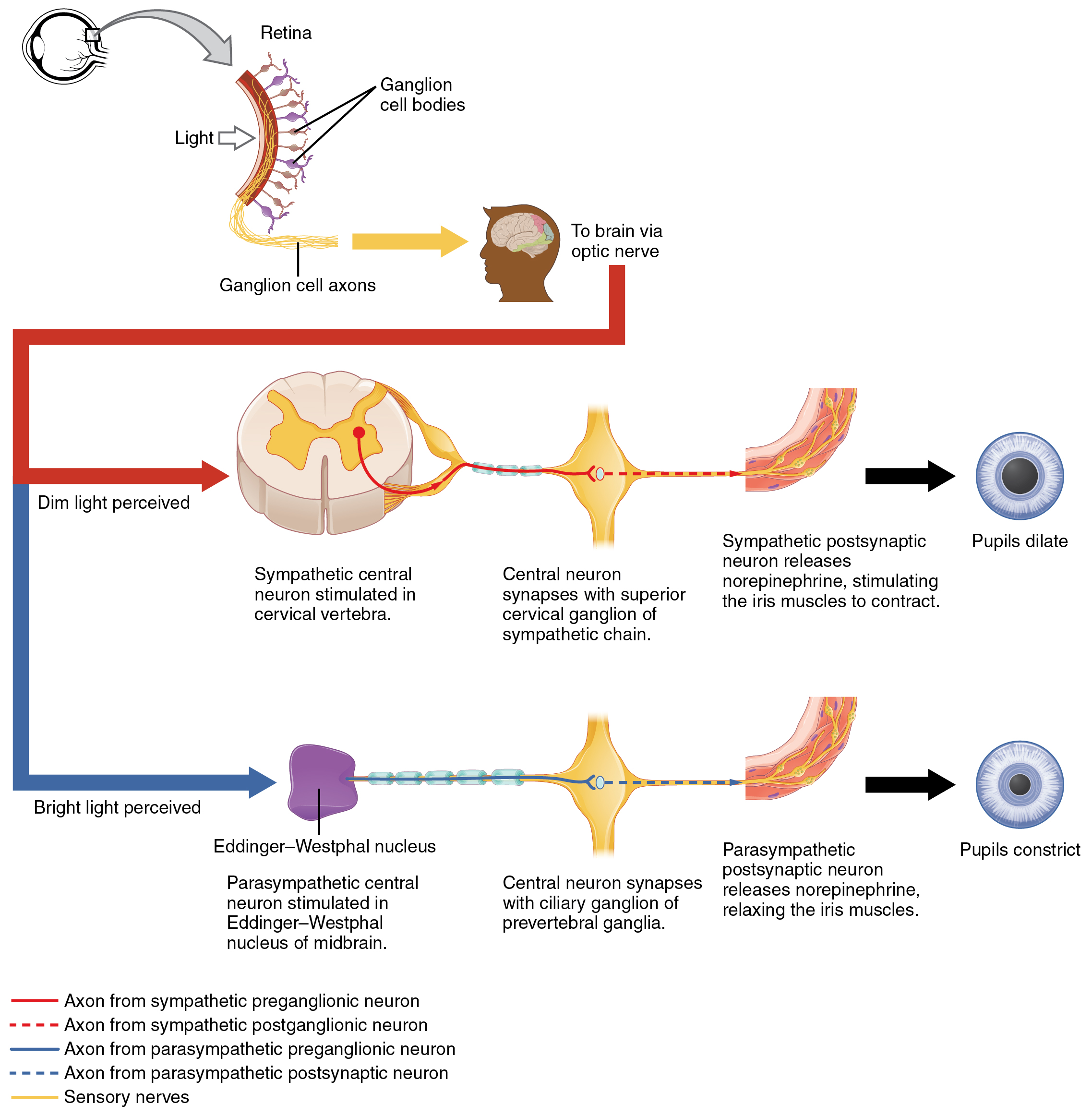
pupil reflex: CN2 light sensation-->CN3 miosis
diplopia/nystygmus: CN3, CN4, CN6
temporalis m. strength: CN5
facial asymmetry and wrinkles on forehead: CN7
- central: wrinkle loss
- peripheral
uvula deviation: to the "good" side, CN9
tongue deviation: to the "bad" side, CN12
SCM power: CN11 (little value for localization of lesion)
Barbinski sign: null-->also abnormal!
 |
| http://epomedicine.com/clinical-medicine/pathological-reflexes-variations-of-babinski/ |
tendon reflex: hyper-->seek upper lesion
muscle power: check reaction to pain if patient's unconscious
gait/FNF/HKS/: cerebellar signs
speech: eight types of aphasia
- can repeat: transcortical(sensory/motor/mixed)/anomic
- cannot repeat: Broca/Wernicke/conductive/global
5. Localization of lesion
ICA territory: transient monocular blindness
ACA territory: leg > arm
MCA territory: face & arm > leg, aphasia(dominant side), apraxia&neglect (non-dominant side)
PCA territory: alexia w/o agraphia, macula sparing homonymous hemianopia
Vertebral/PICA
Basilar territory: pupil, longtract sign, CNS, cerebellar, lock-in
Cerebellar
Lacunar
6. Stroke management
- check cause of stroke( young stroke? underlying? )
- keep SBP<200 (or 220/120)in acute phase(14 days or less), SBP 140/90 afterwards
- hydration for 3~5 days
- Atorvastatin 80 mg if LDL >100, goal: LDL <70
- aspirin if no contraindications (GI discomfort-> shift to clopidogrel)
- consider NOAC (dabigatran, rivaroxaban, apixaban, edoxaban) or warfarin for AF patients according to histories and clinical symptoms




















{kind=link}